
Students evaluation results
The responses to the questionnaires from the 266 students were included in the study. Respondents were 208 third-year medical students and 58 residents (53 residents in microbiology, 5 in infectiology). The average age of third-year students was 21.0 years, while the average age for residents was 26.2 years. In terms of gender distribution, 65.3% of third-year students and 54.5% of residents were women (Table 3). Among the participants, 6.7% of third-year students (14/208) and 29.3% of residents (17/58) reported having prior experience with BacteriaGame (Q1) (Table 4; Fig. 7).
Table 3 Sociodemographic characteristics of participants
The fluidity of game mechanics (Q2) was rated 4.1/5 by third-year students and 4.4/5 by residents. The game’s ability to mobilize virology knowledge (Q3) scored 4.5/5 for third-year students and 4.3/5 for residents. Additionally, 47.4% (92/194) of third-year students and 41.8% (23/55) of interns reported that some concepts exceeded expected knowledge levels (Q4), while 78.9% (157/199) of third-year students and 60.3% (35/58) of residents found certain viral characteristics or card categories challenging (Q5), particularly those related to diagnostic methods, virus structure (enveloped vs. non-enveloped virus, RNA vs. DNA) and transmission pathways (Table 4; Figs. 7 and 8). Very few students responded (n = 12 for third-year students; n = 19 for residents) to open-ended Q4, “If yes, which one for example”. However, for open-ended Q5 (difficulties encountered with the game), 33.4% (89/266) participants provided a response, while 64.4% (172/266) did not respond or explicitly stated they had no difficulties. For Q6, the majority of participants supported integrating ViroGame with BacteriaGame, with 86.5% of students and 91.4% of residents responding “Yes.” (Table 4; Fig. 7).
Statistical comparisons were conducted to assess differences in responses between third-year medical students and residents. Residents were significantly more likely to have prior experience with BacteriaGame (Q1: 29.3% vs. 6.7%; χ² = 20.66, p < 0.001, Chi-squared test). Residents rated the fluidity of gameplay (Q2) higher than students (mean 4.4 vs. 4.1; p = 0.007, Mann–Whitney U test). In contrast, students gave significantly higher ratings for the game’s ability to mobilize virology knowledge (Q3) compared to residents (mean 4.5 vs. 4.3; p = 0.004, Mann–Whitney U test). Regarding the perception that some content exceeded expected knowledge (Q4), no significant difference was found between students and residents (47.4% vs. 41.8%; χ² = 0.34, p = 0.56, Chi-squared test). However, a significantly larger proportion of students reported encountering difficulties with certain virological concepts (Q5) compared to residents (78.9% vs. 60.3%; χ² = 7.23, p = 0.007, Chi-squared test). For Q6, both groups expressed strong support for integrating ViroGame with BacteriaGame, with 86.5% of students and 91.4% of residents responding “Yes,” and no statistically significant difference observed between the groups (χ² = 0.83, p = 0.36, Chi-squared test).
Table 4 Summary of responses to the post-game questionnaire by groupFig. 7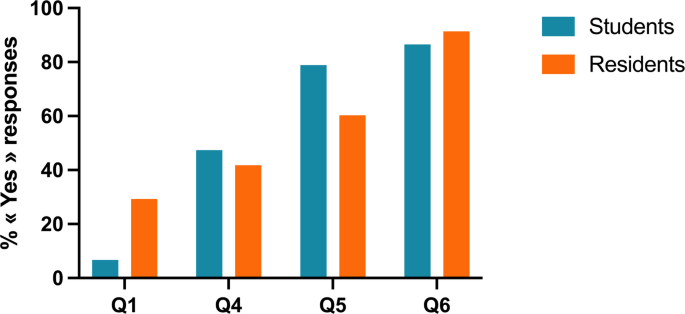
Percentage of students and residents responding “Yes” to questions Q1, Q4, Q5 and Q6.Q1: Prior experience with BacteriaGame Q4: Some concepts exceeded expected knowledge level Q5: I encountered difficulties while playing. Q6: I would like to see the game integrated with BacteriaGame
Fig. 8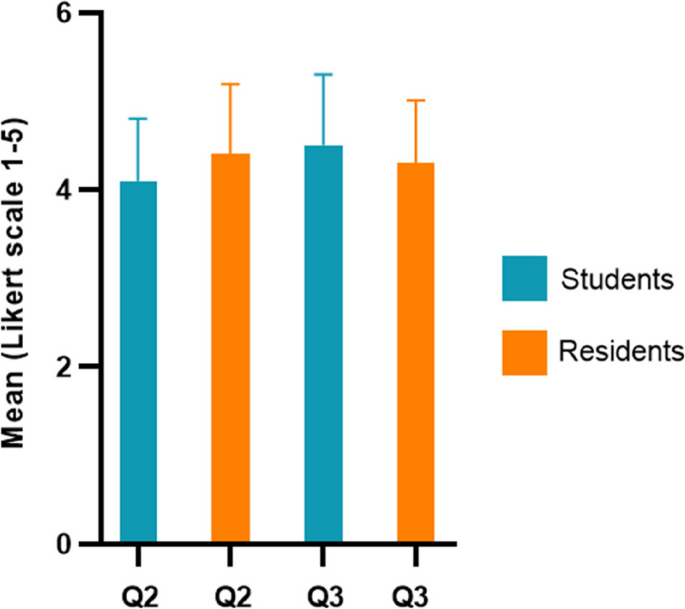
Mean Likert-scale scores [1,2,3,4,5] for Students (blue) and Residents (orange) on three evaluation questions: Q2 (“Did you enjoy the game?“), Q3 (“Did the game help consolidate your knowledge?“). Error bars represent standard deviations
The main difficulties reported by third-year students were related to virus identification and diagnostic aspects (15 mentions), including challenges in associating viruses with their corresponding characteristics and interpreting diagnostic clues. Additionally, 10 mentions highlighted difficulties with card interactions, suggesting that some players struggled with understanding specific game elements or their relationships. Structural and genomic aspects were reported as a challenge by 4 third-year students. Among residents, 20 mentions focused on viral structure and genome, particularly regarding the differentiation of enveloped and non-enveloped viruses. Specific viruses such as Parvovirus B19 and Dengue virus were also cited as difficult by 4 residents.
Open-ended responses Q7 and Q8 highlighted an interest in adding additional viruses, with 37 virus suggestions recorded across both groups: HHV-8 (n = 14), HHV-6 (n = 13), Ebola (n = 6), Zika virus (n = 7), Chikungunya and HTLV (n = 4), Adenovirus (n = 3), Influenza virus (n = 2), West Nile Virus (n = 2), Astrovirus (n = 2), Marburg virus (n = 1), MERS-CoV (n = 1). Residents also suggested a digital adaptation of the game, while third-year students emphasized the need for clearer rules. Finally, 5.6% (15/266) participants left unsolicited positive feedback such as “perfect, release the game, I want to play it!“, “fun way to learn”, “great for revision!“, and “good but quite challenging, you need to know your course well”. These comments highlight the positive reception of the game and its perceived value in engaging students, reinforcing virology concepts and making learning enjoyable.
Supervisor evaluation results
The responses from the 9 supervisors were included in the study. Their evaluation of ViroGame provided positive feedback on both the clarity of the game and its educational impact. The average age of the supervisors was 33.8 years, with varying levels of teaching experience in virology: four supervisors had more than eight years of experience, three had between one and four years of experience, and two had no prior experience in virology teaching. Additionally, five out of nine supervisors had previously supervised BacteriaGame. The supervisors found the rules clear and easy to explain, rating them 3.9/5. The management of a ViroGame session was considered relatively easy, with a score of 4.4/5. Regarding student engagement, they rated how easily students grasped the game mechanics at 4.2/5. In terms of pedagogical effectiveness, the supervisors agreed that ViroGame effectively mobilizes virology knowledge, awarding it an average score of 4.1/5. They unanimously supported the integration of ViroGame into virology courses (100% approval). When asked about the best way to integrate ViroGame into curricula, seven supervisors suggested using it as a revision tool, while two recommended replacing tutorial sessions with the game. Building on this positive feedback, supervisors also offered suggestions to further enhance ViroGame and optimize its use in virology education. To improve gameplay dynamics, they recommended increasing the number of Joker cards to boost student engagement, particularly for those with limited virology knowledge. Some also proposed introducing new mechanics, such as allowing players to exchange virus characteristics, to encourage deeper reasoning. Regarding the potential integration with BacteriaGame, supervisors advised maintaining separate card decks to ensure clarity while balancing the inclusion of both viruses and bacteria. They also noted that while non-virology experts can lead the game, prior training or co-facilitation with a virology expert would maximize its educational impact.